








Types of temporal lobectomy is a surgical procedure performed to treat certain types of epilepsy, especially when seizures originate from the temporal lobe of the brain. It is one of the most commonly performed epilepsy surgeries and often provides significant relief to patients who do not respond well to anti-epileptic medications.
Over the years, different types of temporal lobectomy procedures have evolved to maximize seizure control while minimizing risks to vital cognitive and neurological functions. Thanks to advancements in imaging, surgical techniques, and intraoperative monitoring, these surgeries can now be tailored to each patient’s individual anatomy and seizure profile. From anterior temporal lobectomy (ATL) to selective amygdalohippocampectomy (SAH) and laser interstitial thermal therapy (LITT), each approach offers unique benefits depending on the patient’s condition.
What Is a Temporal Lobectomy?
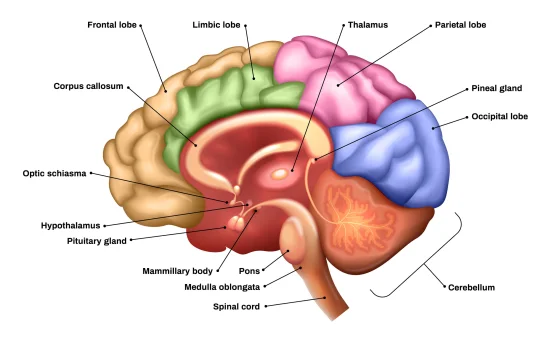
The temporal lobe, located on either side of the brain near the temples, is responsible for functions like memory, language, and emotion. In many patients with temporal lobe epilepsy (TLE), seizures are resistant to medications a condition known as refractory epilepsy.
A temporal lobectomy involves surgically removing a portion of the temporal lobe to eliminate or reduce seizure activity. This procedure is typically considered when :-
-
Seizures are frequent and disabling.
-
Seizures originate from a localized area in the temporal lobe.
-
MRI or EEG shows abnormalities in one temporal lobe.
-
Medications have failed to control seizures.
Types of Temporal Lobectomy
Temporal lobectomy is not a one-size-fits-all procedure. Neurosurgeons tailor the surgical approach based on the patient’s condition, seizure focus, and brain function mapping. The major types of temporal lobectomy include :-
Anterior Temporal Lobectomy (ATL)
Overview :-
Also known as standard temporal lobectomy, ATL is the most common type of epilepsy surgery. It involves removing a portion of the anterior (front) temporal lobe, often including part of the hippocampus and amygdala, which are deeply embedded in the medial temporal structures.
What is Removed :-
-
3–4 cm of the anterior temporal lobe (dominant hemisphere)
-
4–5 cm (non-dominant hemisphere)
-
Amygdala
-
Hippocampus (selectively)
Indications :-
-
Medically refractory temporal lobe epilepsy
-
Clear seizure focus in the anterior temporal lobe
-
Structural abnormalities on imaging (e.g., mesial temporal sclerosis)
Advantages :-
-
High seizure-free rate (60–80% in selected patients)
-
Long-standing success in epilepsy treatment
Risks :-
-
Memory problems (especially in dominant hemisphere surgeries)
-
Language impairment if left hemisphere is involved
Selective Amygdalohippocampectomy (SAH)
Overview :-
This more targeted surgery involves the removal of only the amygdala and hippocampus, sparing much of the lateral temporal neocortex. It aims to minimize cognitive side effects, especially in patients with well-localized seizure foci.
What is Removed :-
-
Amygdala
-
Hippocampus
-
Parahippocampal gyrus (sometimes)
Indications :-
-
Seizures localized to the mesial (inner) temporal lobe
-
Dominant hemisphere epilepsy where memory preservation is crucial
Advantages :-
-
Lower risk of language and memory deficits
-
Suitable for patients with high cognitive demands
Risks :-
-
Technically more challenging
-
Slightly lower seizure-free rates compared to ATL
Tailored Temporal Lobectomy
Overview :-
Tailored lobectomy is a customized surgical approach guided by advanced diagnostic techniques like stereo-EEG, intraoperative brain mapping, and functional MRI. The amount and specific parts of the temporal lobe removed vary based on the patient’s unique seizure network and brain anatomy.
What is Removed :-
-
Varies per individual
-
Could involve parts of neocortex, hippocampus, or amygdala
Indications :-
-
Complex epilepsy cases
-
Non-lesional epilepsy
-
Multifocal seizure origin within temporal lobe
Advantages :-
-
Preserves essential functions
-
Maximizes seizure control with personalized care
Risks :-
-
Requires extensive pre-surgical testing
-
Longer surgical planning period
Laser Ablation or LITT (Laser Interstitial Thermal Therapy)
Overview :-
Laser ablation is a minimally invasive alternative to open brain surgery. Under MRI guidance, a laser fiber is inserted into the seizure focus (usually the hippocampus), and heat is used to destroy the affected tissue.
What is Treated :-
-
Targeted ablation of the seizure-causing area in the temporal lobe
Indications :-
-
Mesial temporal sclerosis
-
Patients unfit for open surgery
-
Those preferring minimally invasive approaches
Advantages :-
-
Smaller incision
-
Shorter hospital stay and recovery time
-
Reduced cognitive side effects
Risks :-
-
Not suitable for widespread seizure activity
-
Long-term success rates slightly lower than ATL
How Is the Type of Temporal Lobectomy Decided?
Before recommending any type of temporal lobectomy, a comprehensive pre-surgical evaluation is conducted, including :-
-
Video EEG monitoring to locate the seizure focus
-
MRI and PET scans for structural and functional imaging
-
Neuropsychological testing to assess memory and language function
-
Functional MRI or Wada test to identify speech-dominant hemisphere
-
Intracranial monitoring in complex cases
Based on these results, a multidisciplinary epilepsy surgery team selects the most appropriate surgical approach for the patient.
What to Expect After a Temporal Lobectomy
Hospital Stay :-
-
Typically 3–5 days for open surgery
-
1–2 days for laser ablation
Recovery Timeline :-
-
Return to non-strenuous activities within 2–4 weeks
-
Full recovery and neurocognitive adaptation may take several months
Seizure Outcomes :-
-
70–80% seizure-free after ATL
-
60–70% seizure-free after SAH or LITT
-
Best results seen in patients with mesial temporal sclerosis
Long-Term Monitoring :-
-
Gradual tapering of anti-epileptic drugs (under supervision)
-
Regular EEG and neurologist follow-ups
Risks and Considerations
While temporal lobectomy is often life-changing for patients with epilepsy, it comes with potential risks, including :-
-
Memory impairment (especially if left-sided)
-
Language difficulty
-
Mood or emotional changes
-
Surgical complications (infections, bleeding, etc.)
It is essential to discuss all potential risks and benefits with your epileptologist and neurosurgeon.
Conclusion
Understanding the types of temporal lobectomy helps patients and caregivers make informed decisions about epilepsy treatment. Whether it’s a traditional anterior temporal lobectomy, a selective approach like SAH, or a cutting-edge technique like laser ablation, each option is designed to improve seizure control while preserving quality of life.












