








Introduction
Dilation and Evacuation (D&E) is a commonly performed medical procedure used to safely remove pregnancy tissue from the uterus during the second trimester, typically between 13 to 24 weeks. It is also used in some cases to manage miscarriage complications or address certain fetal or maternal health concerns. Understanding the different types of dilation and evacuation can help patients make informed decisions, reduce anxiety, and know what to expect before, during, and after the procedure.
What Is Dilation and Evacuation (D&E)?
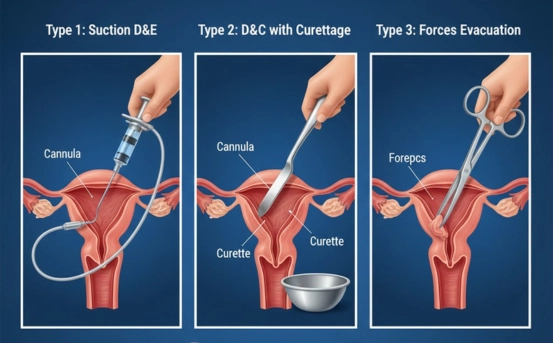
D&E is a surgical procedure that involves dilating the cervix and removing pregnancy tissue using a combination of
- Suction (vacuum aspiration)
- Surgical instruments such as forceps
- Gentle uterine scraping if required
It is performed by experienced obstetrician-gynecologists and is considered safe, effective, and commonly recommended for second-trimester pregnancy management.
Why Are There Different Types of D&E?
Every pregnancy and patient’s health situation is different. Factors such as gestational age, medical history, fetal development, and the reason for the procedure determine which type of D&E is appropriate. The different methods help ensure
- Maximum safety
- Minimal discomfort
- Proper cervical dilation
- Reduced risk of complications
Below are the major types of D&E procedures performed in medical practice.
Types of Dilation and Evacuation (D&E)
- Standard Dilation and Evacuation (D&E) :- This is the most common type of D&E performed during the second trimester. The cervix is gradually opened using medications or osmotic dilators, followed by removal of pregnancy tissue using suction and surgical instruments.
Key Steps
- Cervical preparation (misoprostol or dilators)
- Suction aspiration of uterine contents
- Removal of remaining tissue with forceps
- Possible curettage to clear lining
When It Is Used
- Termination of pregnancy for personal reasons
- Treatment of miscarriage after 13 weeks
- Removal of fetal tissue when development has stopped
Benefits
- Quick procedure (10–20 minutes)
- High success rate
- Low complication risk
- D&E With Osmotic Dilators :- Osmotic dilators, such as laminaria or Dilapan-S, are used to slowly open the cervix over several hours or overnight. This method is especially useful in later gestations or when more dilation is needed.
How It Works
- Thin rods are inserted into the cervix
- They absorb moisture and expand gradually
- Cervix widens safely and steadily
- Surgical D&E performed next day
Ideal For
- Pregnancies between 16–24 weeks
- Patients with tight or unresponsive cervix
- Reduced risk of cervical injury and complications
Advantages
- Allows controlled, gentle cervical dilation
- Improves procedure safety
- D&E With Medication-Only Cervical Preparation :- In this method, medications like misoprostol or mifepristone are used to soften and dilate the cervix without the use of osmotic dilators.
Common Medication Protocols
- Misoprostol tablets inserted vaginally or taken orally
- Mifepristone given 24 hours prior for better dilation
- D&E performed once cervix is adequately dilated
When It Is Recommended
- Earlier in second trimester (13–16 weeks)
- Patients preferring non-dilator methods
- When quicker cervical preparation is required
Benefits
- No insertion of cervical rods
- Good for patients who prefer same-day preparation
- Shorter waiting time compared to dilators
- Induction Followed by D&E (Hybrid Approach) :- This method combines labor induction and D&E. It is used in complex situations where medication begins the pregnancy expulsion process, but surgical evacuation is needed to complete the procedure.
How It Works
- Labor-inducing medications start the process
- Partial expulsion occurs naturally
- D&E completes the removal of remaining tissue
Indications
- Certain fetal anomalies
- Severe maternal health risks
- When induction alone may be prolonged or incomplete
Advantages
- Improves safety for medically complicated cases
- Reduces procedure duration
- Helps avoid prolonged induced labor
- Late Second-Trimester D&E :- For pregnancies closer to 24 weeks, additional steps are taken to ensure safe dilation.
This may involve
- Multiple osmotic dilators
- Combination of misoprostol + laminaria
- Overnight or two-day preparation
Why It’s Needed
- Cervical tissue naturally stiffer later in pregnancy
- Greater safety requirements
- Reduced risk of cervical laceration or heavy bleeding
Best For
- Higher gestational ages
- Patients with prior cesarean deliveries
- Pregnancies with fetal anomalies or maternal complications
- Dilation and Extraction (D&X) :- D&X is a less common and more specialized form of D&E performed in select medical situations, often when the fetus is at a more advanced second-trimester stage.
Features
- Requires extensive cervical dilation
- Removal of fetal tissue intact
- Performed only when medically indicated
Not Routinely Used For
- Standard second-trimester terminations
- Early second-trimester miscarriages
Used For
- Certain fetal anomalies
- Placental or structural complications
How Doctors Choose the Appropriate Type of D&E
The choice depends on multiple medical and personal factors, including
- Gestational age
- Patient’s medical history
- Cervical condition
- Reason for procedure
- Urgency or timing constraints
- Personal comfort and preference
Discussing these details with a gynecologist is essential for a safe and informed experience.
What to Expect Before a D&E
Before the procedure, healthcare providers typically perform
- Pelvic ultrasound
- Blood tests
- Clinical history evaluation
- Cervical preparation using medications or dilators
Patients may also receive instructions on
- Fasting
- Transportation
- Pain management
- Counseling or emotional support
Recovery After a D&E Procedure
Most people recover within a few days. Typical experiences include
- Mild cramping
- Light bleeding
- Fatigue
- Emotional sensitivity
Doctors usually recommend
- Avoiding heavy lifting for 48 hours
- Abstaining from intercourse or tampon use for 1–2 weeks
- Following up if bleeding becomes heavy or prolonged
Is D&E Safe?
Yes. When performed by trained specialists, D&E is considered one of the safest second-trimester medical procedures with low rates of complications. It is often safer than prolonged labor induction at similar gestational stages.
Conclusion
Understanding the types of Dilation and Evacuation procedures helps patients feel empowered, informed, and prepared. Each type of D&E is designed to prioritize safety, comfort, and medical precision depending on individual needs. If you or someone you know is considering a D&E, consult a qualified gynecologist who can guide you through the best option based on your medical situation and preferences.












