








Introduction
Coronary artery disease (CAD) remains one of the leading causes of morbidity and mortality worldwide. Among the various treatment approaches available, Coronary Artery Bypass Grafting (CABG) continues to be a gold-standard surgical solution for patients with severe or multi-vessel coronary blockages. One of the most advanced and durable techniques used in CABG is Bilateral Internal Mammary Artery (BIMA) grafting. BIMA grafting utilizes both the left and right internal mammary arteries to restore blood flow to the heart muscle. Compared to single internal mammary artery grafting, BIMA offers improved long-term survival, better graft patency, and reduced need for repeat interventions. This blog explores the different types of BIMA bypass surgery, their surgical techniques, advantages, and patient considerations.
What Is BIMA Grafting?
Bilateral Internal Mammary Artery (BIMA) grafting involves harvesting both internal mammary arteries left (LIMA) and right (RIMA) from the chest wall and using them to bypass blocked coronary arteries. These arteries are preferred due to their resistance to atherosclerosis, excellent long-term patency rates, and ability to adapt to increased blood flow demands. BIMA is often recommended for younger patients, diabetics with good wound-healing potential, and individuals with multi-vessel coronary disease requiring long-term durable outcomes.
Why Are There Different Types of BIMA Bypass Surgery?
The types of BIMA grafting are determined by
- The method of harvesting the arteries
- The configuration and routing of grafts
- Patient anatomy and disease severity
- Surgeon expertise and surgical goals
Each type offers specific benefits and is selected based on patient-specific clinical factors.
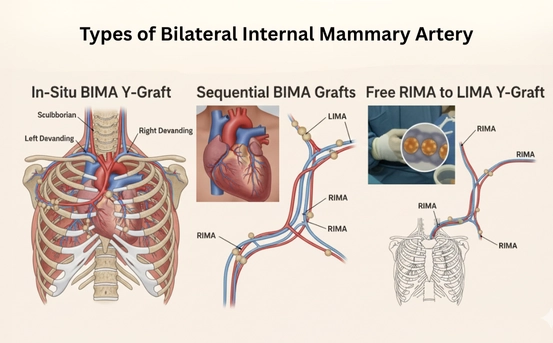
- In-Situ BIMA Grafting :- In-situ BIMA grafting is the most commonly used and anatomically natural form of BIMA. In this technique, both internal mammary arteries remain connected to their original blood supply at the subclavian arteries.
Key Features
- LIMA is typically grafted to the Left Anterior Descending (LAD) artery
- RIMA is routed to the right coronary artery or circumflex branches
- Arteries maintain native blood flow
Advantages
- Excellent long-term patency rates
- Lower risk of graft failure
- Physiological blood flow dynamics
Limitations
- Technical complexity in routing RIMA
- Limited reach in some patients
- Skeletonized BIMA Grafting :- Skeletonized BIMA refers to the technique of harvesting the internal mammary arteries without surrounding muscle and connective tissue. This approach allows greater graft length and preserves chest wall blood supply.
Key Features
- Arteries are carefully dissected free
- Minimal damage to surrounding tissues
- Improved sternal blood flow
Advantages
- Reduced risk of sternal wound infection
- Increased graft length and flexibility
- Ideal for diabetic and obese patients
Limitations
- Requires high surgical expertise
- Slightly longer operative time
Skeletonized BIMA has become increasingly popular due to its safety profile and versatility.
- Pedicled BIMA Grafting :- In pedicled BIMA grafting, the internal mammary arteries are harvested along with surrounding veins, muscle, and connective tissue as a single unit.
Key Features
- Traditional harvesting technique
- Easier and quicker than skeletonization
- Provides robust arterial blood flow
Advantages
- Technically less demanding
- Widely practiced and well-studied
Limitations
- Higher risk of sternal wound complications
- Less graft length compared to skeletonized BIMA
This type is often used in patients with low infection risk and good bone health.
- Composite (Y or T) BIMA Grafting :- Composite BIMA grafting involves creating a Y- or T-shaped configuration where one internal mammary artery is connected to the other, allowing multiple coronary targets to be bypassed using arterial grafts.
Key Features
- LIMA serves as the main inflow graft
- RIMA is attached as a side branch
- No need for aortic manipulation
Advantages
- Reduced risk of stroke
- Allows total arterial revascularization
- Excellent for multi-vessel disease
Limitations
- Complex surgical planning
- Dependent on adequate inflow from LIMA
Composite BIMA is ideal for patients with extensive coronary blockages.
- Free RIMA with In-Situ LIMA :- In this technique, the right internal mammary artery is detached completely and used as a free graft, while the left internal mammary artery remains in situ.
Key Features
- Free RIMA is anastomosed to the aorta or LIMA
- Provides flexibility in reaching distant coronary vessels
Advantages
- Extended reach for complex coronary anatomy
- Useful when in-situ RIMA is not feasible
Limitations
- Slightly higher risk of graft failure
- Requires additional anastomosis
This type is chosen when anatomical constraints limit standard BIMA use.
- Sequential BIMA Grafting :- Sequential BIMA grafting uses a single internal mammary artery to supply blood to more than one coronary artery through multiple anastomoses.
Key Features
- One artery bypasses multiple blockages
- Efficient use of arterial grafts
Advantages
- Reduced number of grafts required
- Preserves other conduits
Limitations
- Dependent on good arterial flow
- Failure may affect multiple coronary territories
This approach is carefully selected based on coronary anatomy.
Patient Selection for BIMA Types
Not every patient is an ideal candidate for all types of BIMA grafting. Surgeons consider
- Age and life expectancy
- Diabetes and obesity status
- Bone health and infection risk
- Extent of coronary artery disease
Proper selection ensures optimal outcomes and minimizes complications.
Long-Term Outcomes of BIMA Grafting
Multiple studies have shown that BIMA grafting
- Improves long-term survival
- Reduces repeat revascularization
- Maintains superior graft patency
- Enhances quality of life
When performed using the appropriate type, BIMA offers lasting benefits compared to vein grafts.
Conclusion
Bilateral Internal Mammary Artery (BIMA) grafting represents a significant advancement in coronary bypass surgery. With various types ranging from in-situ and skeletonized techniques to composite and sequential grafting surgeons can tailor the approach to each patient’s anatomy and clinical needs.
Understanding the types of BIMA grafting helps patients make informed decisions and highlights the importance of choosing experienced cardiac surgical centers. When applied correctly, BIMA remains one of the most durable and life-saving strategies in modern cardiac surgery.












