Vitrectomy surgery is a delicate procedure in which a surgeon removes the eye’s own jelly-like vitreous humor from its center. The vitreous normally fills the space behind the lens and keeps the globe firm. Once the cloudy gel is gone, the surgeon substitutes it with sterile salt water, a gas bubble, or silicone oil so that the eye retains its shape and the retina stays flat. Normally, only doctors who specialize in the vitreous and retina perform the operation. In the United States about 225,000 of these surgeries are done each year, and the total keeps growing as clinicians discover new conditions that benefit from the technique.
Why Vitrectomy Surgery is Needed
Surgeons turn to vitrectomy surgery when serious trouble in the retina or the overlying vitreous puts central or peripheral vision at risk. Among the most common indications are:
- Diabetic retinopathy:- In advanced diabetes, the retina may sprout abnormal new blood vessels that spill or ooze fragile fluid into the surrounding gel. The resulting vitreous hemorrhage clouds vision, and vitrectomy surgery wipes away the blood, clears the path for healing, and stops damage to the delicate retinal tissue.
- Retinal detachment :- when the light-sensitive inner layer of the eye tears or lifts away from its backing – demands urgent repair. During vitrectomy, the surgeon enters the eye, trims the cloudy gel, and uses laser or freezing spots to flatten and bond the retina.
- Vitreous hemorrhage can flood the jelly:-like chamber after diabetes, blunt impact, or existing retinal tears. Since the fresh blood blocks light and produces sudden shadows, vitrectomy surgery is required to remove the haze and restore normal pathways.
- Severe eye injury-whether a blow, shard of glass, or a needle, or a serious infection such as endophthalmitis-leaves debris and cells drifting in the vitreous. The same procedure clears this waste and, if necessary, delivers concentrated antibiotics right to the endangered retina.
Tiny holes, slick epiretinal membranes, or square puckers that form in the macula can warp central vision. During vitrectomy surgery the surgeon gently peels these off and releases tugging tissue, frequently allowing straight lines to return.
In very rare cases fragments, fine aspirated material, or stray scar tissue remaining after routine cataract surgery block the rear sight line. vitrectomy surgery then clears the obstruction and prevents delayed swelling or detachment of the retina.
Untreated, all of these issues can cause severe and permanent vision loss. Prompt vitrectomy, tailored to the problem, is often the safest route to a clear view of the retina and lasting visual improvement.
Signs that Might Point to a Need for Vitrectomy Surgery
Some warning signs appear when the vitreal and retinal tissues are under threat and may call for a vitrectomy. Watch for:
- Flashes of light: Sudden brief sparks or arcs seen in the side or center of vision. These are called photopsia.
- Floaters: Fresh specks, thread-like lines, or cobwebs drifting across straight ahead. They may be clumps of gel, blood, or debris moving with the eye.
- Blurred or lost vision: A patch of haziness or rapid drop in clarity, as if an invisible veil has fallen. It can signal that fluid or blood in the vitreous is blocking light to the retina.
- Dark curtain or shadow: An opaque curtain sliding down over part or all of the visual field. This well-known sign points strongly to possible retinal detachment.
- Eye pain, redness, or discharge: Severe pain, marked redness, and yellow or green drainage may mean endophthalmitis, a serious inside-eye infection. Treatment often begins with immediate vitrectomy.
Any of these symptoms-especially a sudden surge of floaters, flashes, or vision drop-demands prompt attention from an eye specialist. The underlying cause, whether tear, bleed, or detachment, rarely improves without quick, expert care.
Causes Leading to the Need for Vitrectomy Surgery
Surgeons plan a vitrectomy each time symptoms point to damage inside the eye that only glassy-body removal can repair. The chief triggers include:
- Aging and vitreous changes: Over decades, the jelly-like vitreous shrinks, detaches from the retina, and pulls at its edges. That tug can rip tissue, turning small flashes of light into serious tears or detachments.
- Diabetes and vascular disease: High blood-sugar and pressure weaken retinal vessels, provoking diabetic retinopathy and fragile new growths. Tiny bleeds or dense scar tissue from these leaks often force the surgeon to scrape and seal with vitrectomy.
- Trauma or injury: Blows, punctures, or rapid pressure swings-brought by coughing or straining-can tear vessels and chill the retina. The debris, bone chips, or fresh clots left behind mandate immediate clearing to save vision.
- Inflammation and infection: Severe inflammation, such as endophthalmitis after cataract work, clouds the chamber with cells and pus. A swift vitrectomy washes out this sludge and creates a path for lifesaving antibiotics to enter.
- Retinal diseases: Disorders like wet macular degeneration or epiretinal membranes pull and bend central vision, forming holes and distortions. Surgical release of scar tissue smooths the surface and restores steadiness to the fragile nerve layer.
- Congenital or developmental factors: In preterm infants, retinopathy of prematurity promotes poor retinal vessel growth and scar formation. As a result, traction forces on the retina can lead to detachment, often managed with vitrectomy surgery and adjunct procedures.
- Each of these conditions jeopardizes either the tissue health of the retina or the overall transparency of the eye. The surgery is therefore customized to the underlying issue, such as peeling off scar tissue in diabetic retinopathy or resecuring a torn retina.
How Vitrectomy Surgery is Diagnosed
The decision to perform a vitrectomy surgery begins with a complete eye assessment. An ophthalmologist, frequently a subspecialist in retinal diseases, dilates the pupils and examines the vitreous and retina with a slit-lamp and indirect ophthalmoscopy. During this visit, the doctor searches for tears, detachments, bleeds, or abnormal membranes. To clarify findings, additional testing may include:
- Optical coherence tomography (OCT): This handheld or stationary scanner captures cross-sectional images of the retina, showing macular tears, edema, and epiretinal membranes with remarkable clarity.
- Ultrasound imaging: An ocular scan sends sound waves into the eye and receives echoes to outline hidden structures. It is invaluable when cataract or blood obscures the view and can confirm detachment or hemorrhage that direct observation fails to reveal.
- Fluorescein angiography involves injecting a bright-yellow dye that travels through the blood vessels of the retina. Under a special blue filter, the specialist can spot leaks and newly formed, fragile vessels in diabetic retinopathy, often triggering a recommendation for vitrectomy. In more complicated cases, the clinic might rely on fundus autofluorescence or indocyanine green angiography to map areas of damage across the entire retina. These images work together with other tests to outline the full extent of injury before a treatment plan is set.
- Ultimately, the decision to proceed with surgery rests on how well the symptoms match what the doctor sees. If scans reveal a tear, full detachment, stubborn bleeding, or a finding unlikely to self-repair, the ophthalmologist will advise moving forward with vitrectomy.
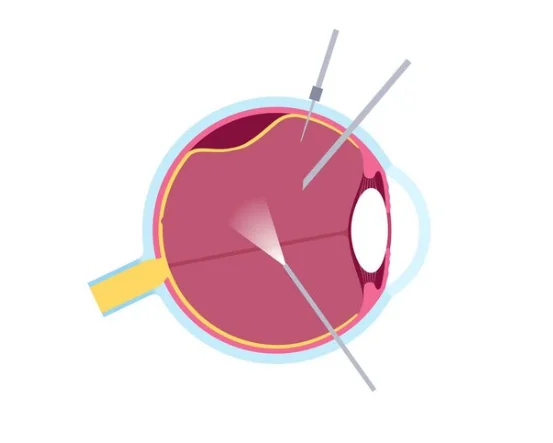
- Vitrectomy is normally done as an outpatient procedure, with the eye still and the patient under light sedation, local anesthetic, or, on occasion, general anesthesia. Key phases in the operation include:
- Preparation: Patients follow fasting instructions and arrange a ride home. The eye is numbed, its pupil widened, and a small speculum keeps the lids open.
- Incisions: The surgeon makes one or two tiny openings in the sclera. Finely gauged instruments-commonly 23, 25, or 27 gauge-allow entry without stitches. During the procedure most people feel only mild pressure or warmth, not sharp pain.
- Vitreous removal: Using the small openings, the surgeon cuts and suctions out the clear jelly of the eye. Any strands of scar tissue or thin membranes on the retina may be peeled away. Through the same ports the team delivers a laser beam or a quick freeze to seal tears or quiet overgrown blood vessels.
- Fluid replacement: Once the old gel is gone, the cavity is filled with sterile salt water, a measured gas bubble such as SF6 or C3F8, or thick silicone oil. The bubble or oil holds the retina flat while healing occurs, and over days the eye gradually swaps the artificial fluid for its own.
- Closing: Most of the tiny cuts seal on their own, though a few may need micro stitches. A drop of antibiotic gel is placed, and the patient often wears a light patch for comfort and protection.
Recovery: After retinal surgery, you rest briefly in a recovery room and usually return home the same day. Key recovery steps include:
Head positioning: If the surgeon used a gas bubble, youll need to hold your head in the prescribed position-often face-down-for several days so the bubble presses against the retina Cleveland Clinic. When silicone oil is used, strict positioning is not needed, but plan on a second outpatient procedure to remove it.
Medications: Youll use the ordered eye drops-antibiotic and steroid drops-to prevent infection and calm swelling.
- A clear patch or rigid shield is often worn during the first night. Activity: For roughly two weeks, avoid strenuous exercise, heavy lifting, and rapid bending.
- Driving is forbidden until your vision stabilizes and the doctor clears you. Depending on the job, most people need 2 to 4 weeks away from work or school to rest Cleveland Clinic.
Follow-up: Close check-ups are vital. Youll return the day after surgery so the surgeon can review healing, test eye pressure, and confirm that the retina is still attached. Call the office right away if vision worsens or if severe pain develops.
Visual recovery after vitrectomy surgery varies from patient to patient. Blurred vision is common in the days after surgery, and a gas bubble, if present, will initially obscure most of the field; patients can expect gradual top-to-bottom clearance as the bubble slowly dissipates over weeks. Even without a bubble, the eye may look red and slightly swollen at first. Over the next few days to weeks, vision typically sharpens again as the chamber refills with natural fluid. To support this healing process, it is vital to use prescribed eyedrops and follow instructions on head positioning and activity.
Thanks to modern small-gauge instruments, most vitrectomies are performed in an outpatient setting and tolerated well. Discomfort is usually mild, and many people notice steady improvement in vision as the eye continues to heal. That said, complete recovery may still require several weeks or, in some cases, months, depending on the original condition that warranted surgery.
Conclusion
Vitrectomy surgery remains one of the most effective procedures for a wide range of sight-threatening disorders. By removing cloudy or damaged vitreous gel and addressing any retinal tears or scar tissue, surgeons can save or even restore vision that otherwise might be lost. Newer surgical techniques, coupled with gentle instrumentation, have shortened theater times, reduced risk, and allowed many patients to be discharged on the same day with only basic aftercare.
Anyone noticing warning signs such as flashes, floaters, a curtain across the field of vision, sudden blurring, or intense eye pain should see an ophthalmologist without delay. Catching the problem early is vital because many retinal disorders are far easier to treat before lasting harm sets in, and most surgical options spare vision when applied promptly. If an operation is required, vitrectomy surgery frequently becomes the preferred route and usually offers the greatest opportunity to restore sight. Success hinges on strictly following postsurgical directions-medications, head position, scheduled returns for exam-so do not overlook them. When care is timely and recovery proceeds as planned, patients often gain substantial improvement in vision after the procedure.